GSI
A Multi-Tiered Plan
to Tackle Snakebite

Neglected No More
In just a few short years, snakebite envenoming has snowballed from a historically ignored crisis, to a rapidly growing global health movement. While the crisis remains, GSI’s mission is to ensure the momentum continues.
It could be a child walking to school in a village near Chennai, India. A mother gathering cooking wood, or a herdsman guiding livestock in any part of sub-Saharan Africa. A rice paddy farmer in Vietnam, or an indigenous elder in Ecuador. Men, women and children going about their daily lives in the poorest and most rural parts of the world faced with an unexpected and avoidable accident. Every day we hear heartbreaking stories of lives ended or ruined by a snakebite.
In the United States, snakebites are rarely fatal thanks to well-trained doctors, abundant antivenom, accessible transport and most often, insurance-covered treatment. But in 168 tropical and subtropical countries where more than 7,400 bites occur daily (5 million annually) it’s the POLAR OPPOSITE! People in snakebite endemic countries regularly witness the devastation of suffering neighbors and list a bite from a snake among their greatest fears.
The solutions to turn the tide are not complicated. After all, snakebite is preventable and treatable. Join us, as we do our part to bring decades of combined expertise to fill critical gaps by implementing tangible, life-saving programs. Everything we do aligns with the World Health Organization strategy to reduce snakebite death and disability by half, by 2030.

THE GLOBAL SNAKEBITE CRISIS
BY THE NUMBERS
The numbers are shocking.
From the lives claimed to the limbs lost, learn more about the toll of snakebite by clicking on the tiles below.

Photo Courtesy: Lillian Lincoln Foundation
Jackson and Esme Kiplagat stand over the grave of their daughter Scola who quickly succumbed to a cobra bite while sleeping in her rural Kenyan home. Twin sister Chepchirchir, seen here in her mom’s arms, was also bitten that fateful night. The family scrambled to find a motorbike to get to the nearest hospital. After the first two health facilities had no antivenom in stock, they arrived at a third, five hours later. Chepchirchir remained in hospital for two months, which put the family into dire financial straits. This burden has continued, as Chepchirchir, now 9, has a severely deformed hand, is blind, unable to walk and suffered severe organ damage. She must be cared for 24/7.
138,000
global deaths
A high-end estimate of the men, women and children who lose their lives each year. Rural dwellers, many of them under 30, make up the greater majority of the mortality, mostly in sub-Saharan Africa, SE Asia, and Latin America.
138,000
global deaths

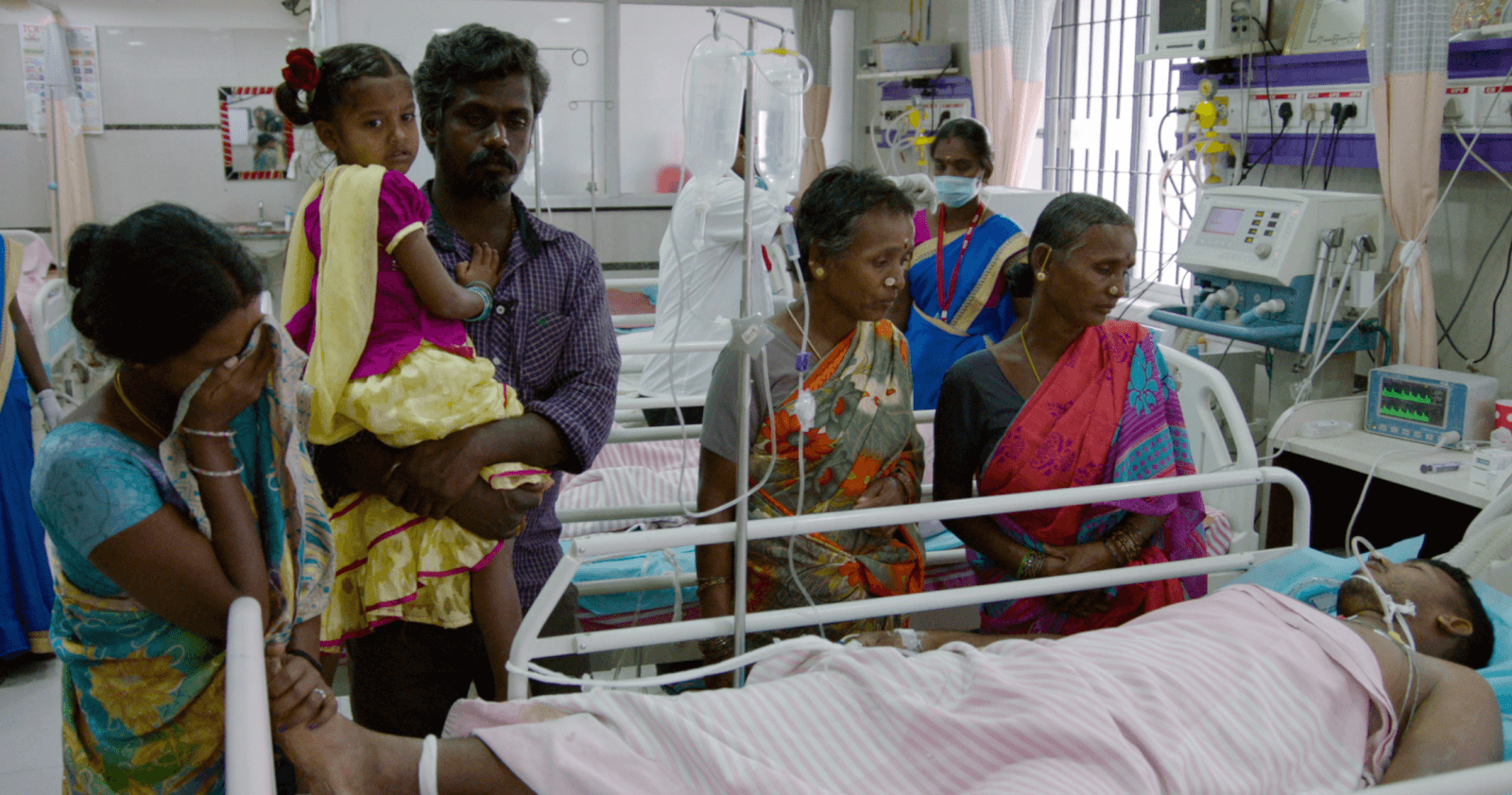
A mother watches over her child on a ventilator following a snakebite in Papua New Guinea. Photo: David J. Williams
Recent increased efforts to collect robust data in hospitals and communities will provide more accurate figures, but under-reporting globally remains problematic. Estimates of 81,000-138,000 deaths annually, reported in literature, are based on extrapolation from limited data. For many countries, there is no formal data collected on snakebite incidence and its outcomes, to inform better estimates.
GSI supports WHO’s call for improved epidemiological surveillance to improve national, regional and global estimates.
Source: PubMed
400,000
disabilities
A disfigured hand, an amputated limb, irreversible chronic renal failure, blindness and even PTSD are just a few of the lifelong physical and psychological effects suffered by those lucky to survive.
400,000
disabilities

Sundai’s arm was amputated following a snakebite while using a latrine at night. His dreams of furthering his education were dashed by crippling fear of another bite occurring. Photo: Lillian Lincoln Foundation
Lack of access to effective and affordable treatments, prehospital care and transport, poor training of health care workers and insufficient awareness in communities about snakebite prevention and treatment options drives this staggering figure.
5.4 MILLION
People are bitten each year and of those, 2.75 million involve bites by venomous snakes.
5.4 MILLION
Annual Venomous Bites

20
neglected tropical diseases (NTDs)
20
neglected tropical diseases (NTDs)
Before his passing, former UN Secretary-General Kofi Annan joined our global effort and called snakebite “the most neglected of all neglected tropical diseases” and “the biggest public health crisis you’ve likely never heard of.” The voice of the respected statesman helped snakebite gain momentous recognition. After all, Mr. Annan knew the plight suffered by those in his home country of Ghana.
In 2017, the WHO designated snakebite envenoming as a category A neglected tropical disease (NTD), adding it to a portfolio of other NTDs such as leishmaniasis, leprosy and trypanosomiasis. Even with other familiar NTDs like dengue (25,000 deaths) and rabies (59,000 deaths), more people die from snakebite than all other 19 NTDs combined!
NTDs historically suffered from a lack of prioritization and resource allocation despite the high toll they exact on some of the poorest and most marginalized communities around the world. Getting snakebite envenoming onto this list took powerful advocacy from GSI, Health Action International (HAI), Médecins sans Frontières (MSF), a coalition of countries who suffer high snakebite burdens, along with many other stakeholders.
58,000
deaths in india
58,000
deaths in india
The family of Periyasamy holds vigil following a bite from a Russell’s viper the previous evening near Krishnagiri, India. Photo: Lillian Lincoln Foundation
India is the global epicenter of snakebite deaths. The mortality rate here, combined with other Asian countries, like Nepal, Bangladesh, Thailand, Vietnam, Indonesia and Myanmar, could be higher than 100,000.
A respected national, community-level study of snakebite deaths in India was 30 times higher than the official snakebite death figure used by the Indian government.
ABOUT THE FRONT PHOTO: This striking photo depicts the human/snake conflict throughout the tropics: the already poor rural farmer harvesting food while a Russell’s viper keeps crop-destroying rodent populations in check. Stepping on a well-camouflaged snake can lead to disaster for the farmer, putting them at risk of losing life or limb, with the possibility of years of financial ruin and loss of the family bread-winner’s future earning potential. GSI works to help communities learn how to mitigate the risk of such tragedies, while living safely alongside snakes. Simple messaging and engagement teach those at risk about becoming more aware of their surroundings, making use of protective footwear or gloves, and taking other simple steps to avert accidental bites.
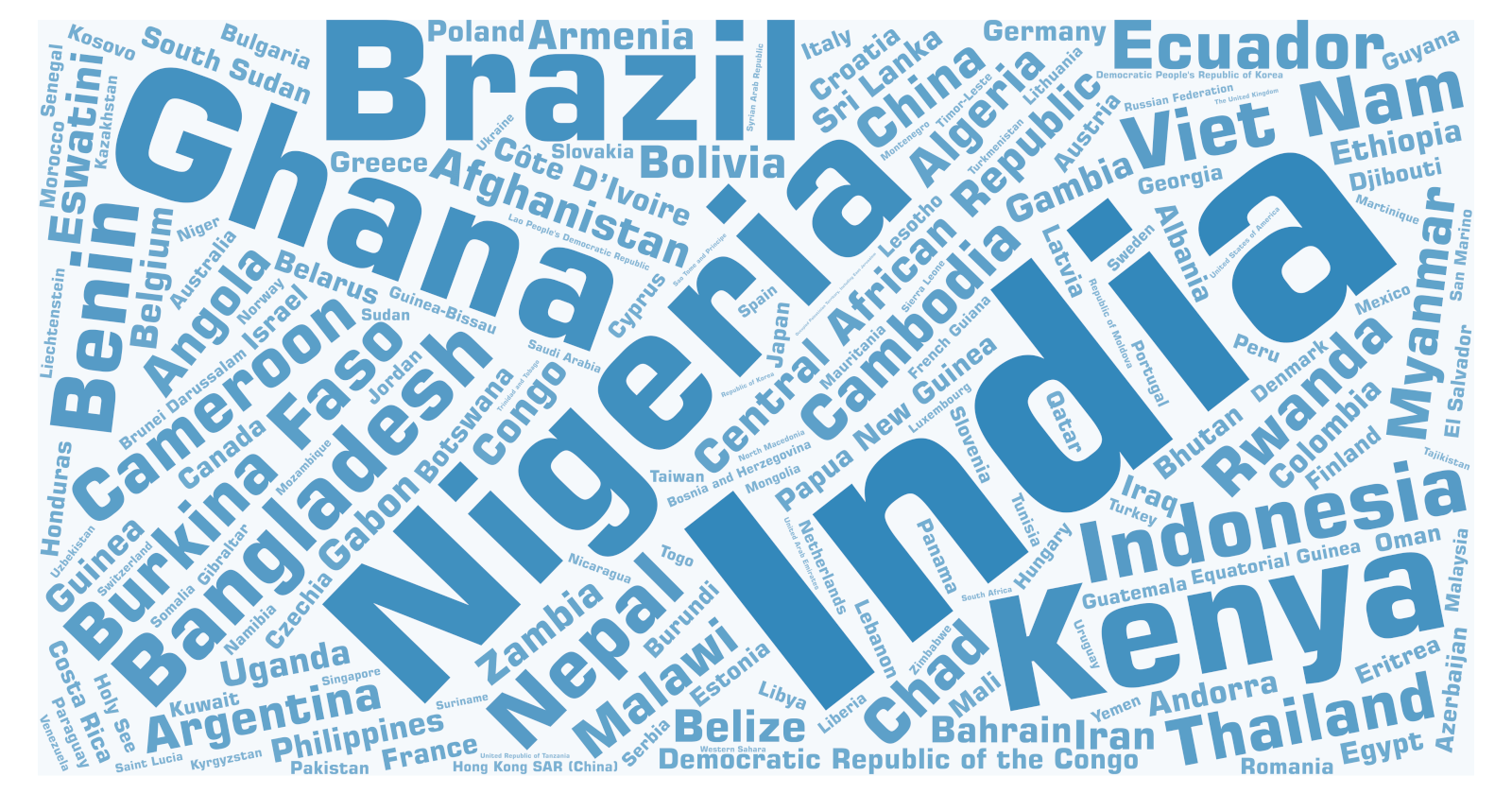
168
Countries
Venomous snakes occur in 168 countries and sovereignties, many of them in tropical and subtropical regions worldwide.
168
Countries
Snakebites also occur in high income, developed nations in Europe, Canada and the United States, Japan and Australia.
$463
The average price per “starting dose” for antivenom in sub-Saharan Africa.
$463
In the United States, a vial of antivenom can cost in excess of $10,000. Antivenoms in sub-Saharan Africa, while much lower and significantly variable, range from $55 to $640, yet some products are considered ineffective at the current recommended doses and may require in excess of 20 vials to neutralize the venoms of some of the most medically-significant snakes.
The cost of antivenoms and overall effective treatments in sub-Saharan Africa, simply put, are out of reach for the already poor snake-bitten patient who may chose alternative forms of treatment from traditional healers, witch doctors and herbalists. Cost becomes a major barrier to receiving effective care, considering the overall price of patient care may absorb days, weeks or months of the family breadwinner’s wages.
While new therapeutics for snakebite are on the distant horizon, antivenom is currently the only solution. Antivenoms in all snakebite endemic countries need to be affordable, available, effective and safe. Many more lives are destroyed by a lack of any of these requirements, in addition to a lack of rehabilitation services which in turn drive families deeper into poverty and poor long-term outcomes. Statistics below from several countries support this viscous cycle.
Brazil
For every one snakebite death, up to 10 survivors are left with permanent disability, including amputations.
West Africa
Only 2.5% who need antivenom have access to it. When available, the cost of treatment is greater than one month’s wages.
India
64.4% pay more than two weeks earnings to pay for treatment. 53.5% sell personal property, land, vehicles, livestock or remove children from school.
Source: PubMed
Bangladesh
61.4% of victims take out loans to cover treatment costs.
Colombia
Only enough antivenom is produced to meet the needs of 75% of victims, leading to declaration of health emergencies by the Ministry of Health.
Source: PubMed
Laos
Supply continuity problems force doctors to treat patients with expired antivenoms.
Source: PubMed
Malawi
Only 26% of surveyed doctors had ever administered antivenom, and 80% of health workers did not know the composition of antivenom.
Source: PubMed
Ecuador
Production discontinued due to lack of political support, adequate investment to maintain facilities and consequential product manufacturing and quality issues.
Source: PubMed
Sri Lanka
79% of victims shuddered economic loss after snakebite. Family members also lost income to care for victims.
Source: PubMed
Burkina Faso
From 2014-2018, none of the 664 victims of snakebite admitted to health centers in Bono-Dioulasso health district had access to antivenom treatment.
Source: PubMed
Morocco
Access to antivenom is a major problem in rural areas where the population can’t afford the cost. This contributed to fatalities and long term morbidities.
Source: PubMed
Benin
Historically, less than 20% of victims in Benin received antivenom and mortality from snakebite cases has been as high as 22%.
Source: PubMed
Zambia
Only 8% of health centers in Ndola district had antivenom available. Lack of central supply and lack of budgets allocated to procure contributed to these shortages.
Source: PubMed
Cameroon
Volume of antivenom available has reduced by 3000% from the 1960’s to 2000. Antivenoms are not available in emergency drug kits of most health workers.
Source: PubMed
Ghana
The case fatality rate increased six-fold after a new antivenom was deployed without having been clinically tested first.
Source: PubMed
72.6%
Of health workers surveyed in Rwanda did not recall receiving training in snakebite management during medical school.
72.6%
96.7% said they hadn’t received any in-service training since graduating either.
In Kenya, Zambia and Uganda, only 8.3-16% of health professionals said they had received snakebite management training.
Heath care workers (HCW’s) who lack training in the treatment of snakebites are typically reluctant to manage patients who present after a snakebite. In communities where HCW’s are poorly trained, patients often avoid attending health facilities and are more likely to rely on traditional healers. When HCW’s are trained or upskilled, antivenom is available, health facilities have basic essential equipment, and when safe, remote retrieval services are in place, as was the case in Papua New Guinea, snakebite victims will confidently seek treatment and word gets out! The case fatality rate in Papua New Guinea dropped from 12.5-25.9%, to less than 1.5% in less than 10 years.
21 HRS
To reach effective snakebite treatment in rural Nigeria
21 HRS
To reach effective snakebite treatment in rural Nigeria

In many parts of the snakebite endemic world, a lack of transportation following a bite means hours on foot. Terrain and land barriers often lead to unfortunate outcomes.
As if the terror of fearing for your life after a snake bite was not enough, imagine having to traverse miles of rough terrain, bush tracks and sometimes impassable roads just to get to the nearest health facility. Every minute of this panic-filled journey comes with not knowing if the health facility will even have the life-saving medicine you need when you do arrive. Unfortunately, it’s also “if” you survive to reach the health center.
A recent study in Nigeria’s remote Kaltungo region surveyed 2,381 patients who had traveled a median distance of 80 kilometers to reach the nearest equipped health facility where health care workers were trained to manage snakebites and where antivenom was in stock. The greater the distance, the higher the likelihood victims would further delay the time to present for treatment by wasting valuable time on traditional first aid methods that had no benefit.
GSI recently visited an area of rural Kenya which exemplifies the obstacles so many snakebite victims endure to get to hospital. These challenges are commonplace throughout countries worldwide with a high burden of snakebite in poorly resourced communities, and highlight the urgent need to improve retrieval options for remote patients.
Our Projects
From GSI’s East Africa Center of Excellence in Kenya, to our India-wide community education programs, to online health worker snakebite training courses, our projects span the globe! Each and every project fulfills key pillars of the WHO Strategy to reduce deaths and disabilities by half, by 2030. Learn more about our current work and how you can support our urgent mission.
GSI's History and Accomplishments
The Origins
Before the Global Snakebite Initiative was formally established, a series of events called for solutions to meet a growing crisis.
2008
Two key meetings set the Global Snakebite Initiative's wheels in motion.
2009
GSI steering committee is established.
2010
Publicizing the problem and a call on WHO for support.
2011
GSI, in collaboration with Australian antivenom producer, CSL launches local research grants.
2012
GSI formally established as a nonprofit in Australia.
2015
The year it all started taking off!

2016
In the door with WHO and a global statesman lends his support.



2017
The next WHO step achieved and the rise of a documentary to put a face on snakebite.

2018
Snakebite envenoming receives unanimous support for WHO programmatic development and implementation.
2019
GSI members contribute to the design and launch of WHO's Snakebite Strategic Roadmap.
2020
GSI breaks ground in Kenya.
2022
GSI-USA is founded.
Will You Band Together with GSI?
We are in need of a committed team of champions to alleviate this unspeakable suffering. Will you band together with GSI-USA’s global network of experts by becoming a GSI-USA Champion today? Your investment in our programs will save lives and limbs, and can change the trajectories of entire families and communities.